9
Medical Marijuana
Robert C. Clarke1 and David W. Pate2
1. PharmTex Consultants, P.O. Box 1158, Ben Lomond, CA
95005, USA
2. International Hemp Association, Postbus 75007, 1070 AA Amsterdam, The Netherlands
Clarke, Robert C.
and David W. Pate. Medical Marijuana, 1994.
Journal of the International Hemp Association 1: 9-12.
Cannabis is a plant with worldwide
distribution, yielding fiber and food, as well as a psychoactive drug. The flowers
have been used as a medicine for millennia. Investigation of its major chemical
components has revealed their utility for the treatment o f a wide variety of diseases. Delta-9-tetrahydrocannabinol
is currently approved as an oral prescription drug for the treatment of the nausea and
vomiting associated with cancer chemotherapy and for appetite stimulation in cases of the
anorexia associated with AIDS. However, many patients find that smoking Cannabis
offers a superior route of administration and therefore illicitly self-medicate.
Introduction
For those not familiar with marijuana and in
need of it for medical purposes, the prospect of consuming an illicit drug may seem rather
daunting. However, marijuana is used by 20-30 million people in the US and many
times that number worldwide, under completely uncontrolled circumstances, with little
apparent harm. It is the world's fourth most popular recreational drug behind
caffeine, alcohol and nicotine. Unlike these latter drugs, Cannabis is not
addictive and no one in the several thousand year history of its use is known to have died
from its effects. The intent of this article is to provide the prospective medical
user with an introduction to this drug as a possible therapeutic option. The basics
of our subject start with the realization that this much-discussed drug, like many of the
others we consume, is from a plant with an interesting natural history.
Cannabis, the plant
Cannabis is a dioecious annual
producing approximately equal numbers of male and female plants. Marijuana comes
from the flower-associated bracts of female Cannabis. The male plant is
much less useful for this purpose. Almost all of the Cannabis found
worldwide is classified as Cannabis sativa. Many taxonomists argue that C.
indica and C. ruderalis are also valid species names (Emboden 1974, Schultes
et al. 1974) although this remains controversial (Small and Cronquist 1976).
However, even accounting for these additional species, 95% of the cultivated Cannabis
in the world would still be classified as Cannabis sativa.
As it grows well at low temperatures, Cannabis
is well adapted to temperate climates (Van der Werf 1994). Ancient northern Asian
and European societies used Cannabis mostly for its fiber and seed. It is
also an aggressive weed plant at higher latitudes worldwide. South Asian and African
cultures used Cannabis mostly for its drug content, and the frost-free climates
allowed more time for development of the psychoactive resin. Intense levels of
ambient ultraviolet radiation and of insect predation in the tropics may also have
contributed to a natural selection for these drug types (Pate 1983). In any case, Cannabis
has evolved into two basic races. Plants grown for fiber and seed are universally
called "hemp". Cannabis grown for its drug content is commonly
called "marijuana" or "drug Cannabis". Its female
flower bracts are covered with numerous small resin glands containing the
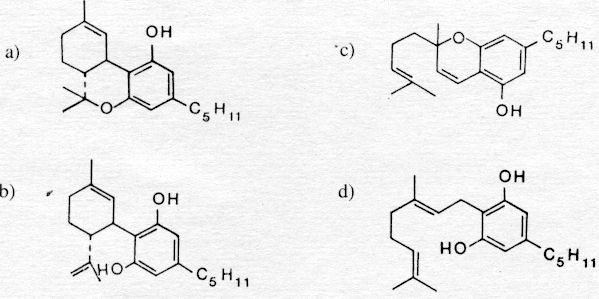
pharmacologically active cannabinoids (Fig. 1) that that are unique to this genus.
Figure 1. Some cannabinoids: a) THC, delta-9-tetrahydrocannabinol; b) CBC, cannabichromene; c) CBD, cannabidiol; d) CBG, cannabigerol.
Most of the psychoactive properties of marijuana can be attributed to its content of a cannabinoid (Fig. 1a) named delta-9-tetrahydrocannabinol (THC). In some literature, it is designated as delta-1-tetrahydrocannabinol due merely to a conflict between two methods of naming chemicals, but it is the very same molecule. Modern hemp varieties are nearly devoid of THC and, therefore, cannot be practically diverted into the drug trade. Hemp has been heavily selected for high fiber content, high stalk yield, high seed yield, and low (<0.3 %) inflorescence thc content (de meijer et al. 1992). Drug-type Cannabis varies widely in thc content from approximately 1-2% in unselected strains to over 10% in the best modern varieties (Watson 1994). It is not feasible to "get high" on hemp, and most marijuana produces very little low-quality fiber. Hemp should never be confused with marijuana, as their roles cannot be reversed.
Cannabis, the medicine
Cannabis has been recognized for
centuries as a valuable therapeutic agent. Folk uses of Cannabis include
treatment of insomnia, inflammation, various psychoses, digestive disorders, depression,
rheumatism, migraine, neuralgia, fatigue, constipation, diarrhea, parasites, appetite
disorders and it has also been employed by women to facilitate childbirth, stimulate
lactation, and relieve menstrual cramping (Mechoulam 1986). These traditions
continue in every region where Cannabis is available. Modern Western Cannabis
users also frequently claim relief from many of these same medical complaints.
Cannabis or THC have been used
experimentally to effectively lower the elevated intraocular pressure of glaucoma (Adler
and Geller 1986) and have shown potential for the treatment of alcoholism (Rosenburg 1976)
and drug dependence (Hine et al. 1975). THC has been used as a bronchodilator for
the relief of asthma symptoms (Graham 1986) and may also be effectively used as an
analgesic for pain relief (Segal 1986). It has even been shown to have antibacterial
properties (Van Klingeren and Ten Ham 1976).
The low toxicity of THC is best indicated by
its widespread use with very few reports of anything even approaching an overdose.
Occasionally, people may get too "high" for their psychic comfort, but their
bodies continue to function fairly normally. The dosage sufficient to kill half of
the organisms tested (LD50) for orally ingested THC is
approximately 1 g/kg of body weight. Simply interpreted, this means an average sized
human would have to consume 50-100 g of pure THC to reach the LD50
level. Since high-potency Cannabis contains approximately 10% THC, a person
would have to eat at least 500-1,000 g of this marijuana before having a 50% chance of
death. A 1 g marijuana cigarette of 10% THC Cannabis contains 100 mg of THC and is
usually shared among several smokers. Clinically effective oral doses for the relief
of nausea start at 5-10 mg. This means that, even accounting for pyrolytic
decomposition and smoke loss, there is a several-thousandfold difference between an
effective dose of THC and a potentially lethal one! For alcohol, this difference is
only about twentyfold. Other common non-prescription drugs, such as aspirin, have
similar relatively narrow margins of safe use. Research into the actions of the
natural cannabinoids led to the creation of many artificial ones based on variations of
their basic molecular structure. However, none of these artificial compounds are
currently approved for medical use in the US. Nabilone proved to be toxic to
laboratory test animals and in 1978, human tests were suspended, although it is available
in Canada, Switzerland and the United Kingdom as Cesamet�.
Levonathrodal, another synthetic cannabinoid analog, was not approved for use in the US,
also following incidents of toxicity in test animals.
Other natural cannabinoids (Fig. 1b-d), such as
cannabichromene (CBC), cannabidiol (CBD) and cannabigerol (CBG) have been shown to have
potential therapeutic value, and can be isolated from both non-psychoactive as well as
psychoactive Cannabis varieties. Epilepsy, multiple sclerosis, dystonias,
and other neurological disorders have been experimentally treated with CBD (Consroe and
Snider 1986). CBD has also been shown to relieve anxiety, especially the minor
anxiety occasionally associated with the medical use of THC (Zuardi et al. 1982).
CBC, CBD, and CBG and related analogs have been shown to have anti-microbial action
(ElSohly et al. 1982, Van Klingeren and Ten Ham, 1976). These non-psychoactive
compounds are generally not restricted by international regulations prohibiting Cannabis
and THC.
Various delivery systems for these
cannabinoids, such as suppositories, time release encapsulation, eye drops, nasal sprays,
aerosols, topical ointments, and transdermal patches will eventually become available.
Several such cannabinoid delivery systems have already been patented (e.g., ElSohly
1990, Hussain 1984).
The only cannabinoid medicine currently
available in the US is a synthetic THC encapsulated in sesame oil (generically known as
"Dronabinol"). It is sold under the trade name Marinol�
as a Schedule II controlled substance (allowing restricted prescription, similar to
morphine and cocaine) and was afforded a narrow, specific legal exemption from the
Schedule I status of other Cannabis products (forbidden from clinical use).
It has been accepted and prescribed in the United States since 1985 as an
anti-emetic to treat the nausea associated with cancer chemotherapy (Levitt 1986).
Use as an appetite stimulant to correct the weight loss related to anorexia in AIDS
patients was approved by the US Food and Drug Administration on December 22, 1992
(Anonymous 1992 ). THC is not a cure for cancer or AIDS, but helps to relieve
suffering and improve quality of life, perhaps prolonging the lives of those afflicted.
THC may also eventually win approval as a general appetite stimulant for anorexia
nervosa and other appetite disorders.
Before other cannabinoids or Cannabis
can become available to patients in the US, they must be similarly rescheduled. This
also applies to the non-psychoactive compounds or even an otherwise identical, but
plant-derived THC medicine! On April 29, 1991, the UN Commission on Narcotic Drugs
decided that delta-9-tetrahydrocannabinol should be transferred from Schedule I
to Schedule II of the 1971 Convention on Psychotropic Substances to facilitate its
therapeutic use. Similar rescheduling in each member country would allow doctors to
prescribe it as a medicine and permit easier research. This has already been
accomplished in England and Germany. Patients claim there is an acute need to reform
the laws concerning other Cannabis products, especially in response to the
medical plight of thousands of cancer and AIDS patients. If economic incentives
could be created by liberalizing outdated anti-Cannabis laws and streamlining new
drug registration and testing procedures for AIDS related medicines, several new Cannabis
medicines would appear on the market within the next few years.
Currently, in the US, the cost of a single dose
of Marinol� ranges between $4.00 and $8.00 and the
average patient cost ranges from $12.00 to $32.00 per day. Since Marinol� is expensive, narrowly prescribed and often less effective
than crude Cannabis preparations, potent sinsemilla-type (seedless) marijuana
remains the most viable form of Cannabis medicine, despite the fact that its
illegality artificially inflates its cost. Physicians learned as much from their
patients and began to publish guidebooks on the appropriate medical use of Cannabis
(e.g., Roffman 1982), which is most often smoked or consumed in baked goods.
In some respects, it may be unfortunate that Cannabis
has played such a prominent role in the American media's coverage of the counterculture
movement since the 1960s. The popularization of Cannabis as the drug of
choice increased its exposure to the general public, but government disinformation
promoted the mainstream culture's confusion of it with hard drugs. It has been
difficult for even the more knowledgeable patients and practitioners to view Cannabis
as a genuine medicine rather than merely a recreational drug. Of course, many
doctors are also reluctant to suggest Cannabis use because it is illegal.
Marinol� is too expensive for many patients to afford
and orally ingested anti-emetics are of questionable value because their application must
be care fully timed to avoid vomiting the drugs. Many patients who both smoke Cannabis
and swallow Marinol� report that THC absorbed through
the lungs offers more immediate relief, better dose titration, fewer side-effects and
shorter duration of action.
Conclusions
For millennia, Cannabis has been used
as an effective medicine. Modern research has revealed the clear potential for this
plant and its cannabinoid products to resume their place in the pharmacopoeia.
Further work is urgently needed to determine how Cannabis can be best utilized as
a clinical tool. Meanwhile, cancer and AIDS patients and members of the medical
marijuana movement have taken responsibility for their own health and self-medicate
without a doctor's prescription.
References